What is immunosuppressive medication in kidney transplant?
Immunosuppressants are drugs or medicines that lower the body’s ability to reject a transplanted organ. Another term for these drugs is anti-rejection drugs.
Why do you need this medication after kidney transplant?
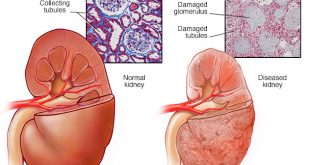
When you get a kidney transplant your immune system will identify the transplanted kidney as non-self or a foreign body. This will trigger the immune system to reject the new kidney and result in damage to the organ.
How do immunosuppressive medications work?
Immunosuppressive medications act to suppress the immune system of the recipient so that it will not react to the transplanted kidney and reject it.
There are a number of drugs used as immunosuppressive agents. These may be divided into induction and maintenance agents. Induction agents are powerful antirejection medicines used at the time of transplant while maintenance drugs are the antirejection medications used for the long term.
Usually, you will need a combination of different immunosuppressive medication.
How long do you need to take the medication?
You will need to be on the medications as long as the graft still functions but the doses of these immunosuppressants are usually slowly decreased over time to help lower the overall risk of side effects.
How are immunosuppressant chosen for a patient?
The combination of medications prescribed is tailored for each individual. Your doctor will study your risk of rejection and balance this against the risk of infection and side effects of the medication when selecting your treatment.
What are the side effects of immunosuppressant medication?
Generally, these medications will cause a higher risk of infection and long-term malignancies . However, different classes of medication have specific side effects .
Classes of immunosuppressant medications:
- Corticosteroids
- Calcineurin inhibitor (CNI)
- Mycophenolate
- Azathioprine
- mTOR (Mammalian Target of Rapamycin Inhibitor)/ Proliferation signal inhibitors (PSI)
- Antibodies
- Antithymocyte globulin – Antithymocyte globulin (ATG) is an immunoglobulin prepared from horse or rabbit sera. It can be used as an induction agent or as a treatment for severe forms of rejection. The antibodies will bind and destroy human leukocytes (white blood cells) . The most common side effect is flu-like symptoms but this agent is also associated with risk of low white cell counts, infections including viral infections, and increased risk of cancer later on.
- Basiliximab – An antibody that blocks the production of T cells. It used as an induction agent and does not increase the risk of opportunistic infections.
Corticosteroids are the most widely used immunosuppressive medication. They are available in intravenous (IV) and oral forms. IV corticosteroids are given prior to transplantation and immediately post-transplantation. After a patient is able to tolerate orally in the post-operation period, the IV steroid will be changed to oral form. The dosage of corticosteroid will be gradually tapered down and kept at a minimum dosage. The action of corticosteroids is non-specific, it blocks both cell and antibody mediated immunity. Some of the side effects of corticosteroids include infections, weight gain, cataracts, new onset diabetes mellitus, osteoporosis, hypertension, dyslipidaemia and muscle weakness.
Two examples of calcineurin inhibitors are cyclosporine and tacrolimus. These drugs primarily inhibit a certain type of white cells known as T cells These cells will become activated once a non-self substance is detected by the body. CNI levels should be monitored with blood tests and the dosage of this class of medication will be adjusted accordingly. Side effects include increased susceptibility to infections, hypertension, gum swelling, new onset diabetes mellitus and hand tremors. Long-term use of CNI can also cause impairment of transplanted kidney function so the levels of these drugs have to be judiciously balanced.
Two forms are available: mycophenolate mofetil and mycophenolate acid. This group of medication inhibits white cell proliferation. The main side effects possible include low white cell counts, stomach upset, and loose stools. They are commonly used in combination with a calcineurin inhibitor and corticosteroids in Malaysia.
This agent inhibits an enzyme that is required for the synthesis of DNA and cell growth. It is used as an alternative to mycophenolate , in a combination of CNI and steroid. Common side effects are marrow suppression and infection.
Two types are used in Malaysia – Sirolimus and Everolimus These agents can be combined with calcineurin inhibitor or mycophenolate. Side effects include stomach upset, oral ulcers and raised serum cholesterol levels Use of mTOR agents in the immediate post-operative period can cause delayed wound healing.
Certain antibody preparations have been used for the prevention and treatment of rejection in kidney transplant. Examples include OKT3, anti-thymocyte globulin (ATG), basiliximab, alemtuzumab, and rituximab.
Below are the statistics of immunosuppressant use in Malaysia for kidney transplant patients
Data from 21st Report of the Malaysian Dialysis and Transplant Registry 2013.

References:
- http://www.interactive-biology.com/3538/what-is-antigen antibody-complex/
- http://www.southafricab2b.co.za/default.cgi/action/viewproducts/productid/216945/productname/Oncology_Anti_Cancer_Drugs/
- https://www.healthtap.com/topics/what-happens-if-i-stop-taking-my-immunosuppressive-drug-suddenly
| Last Reviewed | : | 27 July 2016 |
| Writer | : | Dr. Yaw Chong Hwa |
| Accreditor | : | Dr. Liu Wen Jiun |